PCNL Keyhole surgery for kidney stone
June 23, 2018
, by brojen barman
PERCUTANEOUS NEPHROLITHOTOMY (P.C.N.L.) -keyhole surgery for kidney stones
Because of technology, open surgery for the removal of kidney stones is relatively uncommon. Modern equipment and procedures, such as percutaneous surgery, use x-ray imaging, guide wires and tubes to remove kidney stones. Percutaneous means through the skin. Nephrolithotomy is a surgical cut into the kidney. P.C.N.L. is performed to remove stones that are causing a blockage or to treat ongoing symptoms such as pain and recurrent infection. Recovery time after surgery is much shorter as no large open incisions need to be made unless complications of surgery arise such as excessive bleeding or equipment failure which is rare
.
WHAT DOES THE OPERATION INVOLVE?
Infection and bleeding prior to surgery: In most cases, access to the kidney is done at the start of surgery. Once you are asleep, a thin guide wire is inserted through the back, into the kidney and down toward the ureter. Placement of the wire is done with the aid of x-ray imaging and in some cases special x-ray sensitive dye is also used to ensure the placement is exact.
Once the guide wire is in position, a 1-2cm skin incision is made and a fine hollow tube known as a dilator is threaded over the guide wire down to the stone. Once that has been passed the next sized dilator is taken and threaded in the same way, over the guide wire down to the stone. Each successive dilator is slightly larger than the last and passing these creates a tunnel or tract. A telescopic camera is passed through the tract and its images are conveyed to a television screen. When the stone is in view, if it is small enough, it can be removed using a special basket or grasping device. If it is a larger stone it can be blasted with ultrasound or shock waves or vaporized with the laser into smaller pieces that can then be removed. Once all of the pieces of stone have been removed, a tube, known as a nephrostomy tube, is placed through the tract down into the kidney and it is stitched into place. This is connected to a drainage bag that drains any urine, blood or stone fragments from the kidney. Sometimes a ureteric stent (a thin flexible tube inside your ureter) is placed to allow any stone fragments to pass alongside the stent without blocking off the flow of urine and causing pain. A catheter (a flexible drainage tube) is also placed to drain your urine. The catheter is held in place inside the bladder by a small inflated balloon so it can’t slip out. Apart from the nephrostomy and catheter no other external drains are needed and the only stitches needed are those to hold the nephrostomy tube in place. Depending on the location and number of stones, surgery can take anywhere from 1 to 4 hours to complete and usually involves a one to two night hospital stay.
WHAT RISKS ARE INVOLVED WITH SURGERY?
The risks with percutaneous surgery are less than with open surgery as no large incisions are needed so blood loss and the risk of infection are greatly reduced and recovery time is much shorter. One very slight draw back with percutaneous surgery is that with a tiny incision and instrument surgery being used, the surgeon is limited to what the instruments allow him/her to do. In a small number of cases when numerous or complex stones are involved, other procedures including repeat P.C.N.L may be needed before a patient is completely stone free. With larger stones in the renal pelvis or the upper ureter, access can be more difficult and there is a very slight risk of injury to the ureter during the operation.
This can cause scarring of the ureter, which can narrow the channel. This is known as a ureteral stricture, it is uncommon but if it should occur it is usually easily treated with minor surgery which opens the narrowing.
There is always some bleeding involved with surgery, however if a main artery or vein is involved, large amounts of blood can be lost and open surgery may be needed to control bleeding. This happens very rarely with percutaneous surgery and blood transfusions are uncommon.
The upper part of the kidney sits close to the lungs and on the right side the spleen and on the left the liver. If access to the stone is only possible using a high approach to the upper kidney, the risks of this would be weighed up with the benefits of the Percutaneous approach and surgery would only proceed if the surgeon felt it were in the best interest of the patient. Using a higher approach increases the risk of puncturing any organs close to the kidney. Puncture of the liver and spleen usually causes no ill effects when special precautions are taken, however, puncture of a lung may cause the lung to deflate and a tube may need to be inserted for a short time to re-inflate the lung. All of these complications are very rare and the large majority of patients are stone free after surgery and have a speedy recovery.
YOUR CONSENT
We need your permission for your operation to go ahead. Before you sign the consent form it is important that you understand the risks and effects of the operation and anaesthetic. These will be discussed with you by your doctor and the nurse, should you have any questions, your nurse or doctor would be happy to answer these.
With percutaneous surgery there is a small chance that you may require a blood transfusion either during or after surgery. In the event that you did need a blood transfusion and you want to refuse one, it is vital that you tell your surgeon and nurse prior to your operation.
ABOUT YOUR ANAESTHETIC
You will NOT be allowed to eat or drink anything for at least six hours before your surgery. This includes chewing gum and sweets
This type of surgery requires a general anaesthetic which means you will be asleep throughout the operation and remember nothing of it.
Feel free to discuss any questions with the anaesthetist.
You must not drive any vehicle or operate any machinery for 24 hours after having an anaesthetic. You will have to arrange for someone to drive you home if you go home within 24 hours of your surgery.
YOUR OPERATION
On admission you will be informed of an approximate operation time and prepared for theatre by your nurse. You maybe fitted with T.E.D. stockings that help aid circulation and prevent blood clots, which there is always a slight risk of with surgery. You may also be instructed about special deep breathing and leg exercises that you should do after surgery.
A shave of the surgical site may be required. This is usually done just prior to going to theatre or in theatre itself. You may be given some tablets before theatre. These are charted by your anaesthetist and may include tablets for tension, nausea and pain prevention.
You will be escorted to the theatre, where you will be transferred to the theatre table. Anaesthetic staff will then insert a drip in your arm and will attach various monitoring devices. Once you have been completely prepared and given your anaesthetic, surgery will begin. When the operation is completed you will go to the recovery room for a short while where you will be cared for until you are ready to be transferred to the ward.
AFTER SURGERY
Your nurse will check your blood pressure and pulse regularly. Your wound will be checked for any bleeding and the urine output from your nephrostomy tube and catheter will be monitored closely. You will have a drip in your arm to make sure you receive adequate fluids. This will be removed once you are drinking normally. You can usually drink when your return to the ward and you may eat once you are tolerating fluids.
You may have a P.C.A pump attached to your drip. P.C.A stands for Patient Controlled Analgesia, a computer controlled machine that delivers pain relief through your drip on your command. You will be instructed on the use of the P.C.A. should you have one. You will be given regular pain relieving tablets to keep you comfortable so you may not need a P.C.A pump.
Our aim is to keep you as comfortable as possible, it is important that the nurse know when the pain or discomfort starts so your symptoms can be treated and relieved as quickly and easily as possible. At all times, your nurse is there to help you, please ring your bell if you need assistance and your nurse is not nearby.
ON THE DAY FOLLOWING THE OPERATION:
Your catheter is usually removed 24- 48 hrs following surgery. The balloon of the catheter is deflated which lets the catheter slide out easily and causes little discomfort. Once your catheter has been removed you will be able to get up for a shower and have quiet walks.
If you are eating and drinking normally your drip will come out as long as you do not need further antibiotics or have a P.C.A pump attached.
You may have a burning sensation when passing urine after the catheter is removed. This is because urine is naturally acidic and causes discomfort as it passes any area within the urethra that has been irritated by the catheter. If this happens please tell your nurse who will be able to give you some medication to neutralize your urine and relieve the burning.
Your nephrostomy tube would usually be removed after a check X-ray 48-72 hrs following surgery, You may have some urinary leak from the wound site after the nephrostomy has been removed but it usually settles down on its own.
GOING HOME
Once your catheter and nephrostomy have been removed and you are eating and drinking and passing urine normally, you will be able to go home. In the unlikely event that all of the stone fragments could not be removed and further management is required, you would be advised accordingly for needful management. .
Before leaving the ward you will be given a discharge information letter which contains helpful information for when you get home.
If you have a ureteric stent in place, this may be removed then under local anaesthetic, usually after x-rays to check any stone fragments are passed. A thin flexible, telescopic instrument is passed up the urethra into the bladder so the end of the stent can be grasped and it can be removed.
We will send a letter to your own doctor about your operation and the details of your treatment while you were in hospital
ONCE HOME
Before discharge your nurse will inform you about taking mild pain relievers, should you have any pain or discomfort after you return home.
The internal healing after surgery takes 4-6 weeks. During this time you should avoid any heavy lifting, straining or strenuous activity. Apart from strenuous activities you will be able to continue with your normal daily routines, as you feel able.
You should wash your wound with water only. No soap or powder is to be used directly on your wound until it is healed completely. Your wound would usually be dry within 48 hours of surgery, prior to this you may need to place a small plaster over it to stop any slight ooze marking your clothing.
Avoid becoming constipated by keeping up a good fluid intake and eating fruit and foods high in fibre. If you have problems with constipation you may require a stool softener which you will be able to get from your nearest pharmacy.
Contact your own doctor if
– Your wound becomes red, hot, swollen, painful or continues to discharge.
– your urine becomes cloudy, offensive smelling or you have any other signs of a urine infection.
– you have any concerns at all.
This is routinely a straight forward operation, after which most patients have a speedy recovery and experience little pain.
FURTHER INFORMATION ON HOW DO STONES FORM AND WHAT CAN I DO ABOUT STOPPING THEM FROM FORMING AGAIN?
A stone begins as a tiny particle that is left behind when the urine flows out of the kidney. Over time, particles bond together and the stone becomes larger. The majority of stones are eventually carried out of the kidney into the ureter and down to the bladder, however some stones remain in place within the kidney and continue to grow. When these stones start to block the flow of urine, they can cause pain and infection and this is when treatment is given to remove the stone/s and resolve symptoms. Once a person has had a stone they are more likely to develop another stone compared to someone who has never had a stone before. Most stones are caused by a metabolic imbalance, which is an imbalance of the chemical processes that occur in the body. These imbalances are not life threatening but can lead to a build up of certain minerals within the urine which can form into stones.
The best way to prevent further stones forming is to drink, drink, drink. The best fluid to drink is water, however, any fluid is O.K., but tea and coffee should be restricted. Your daily fluid intake should be between 2-3 litres, or more in the summer months. You will know when you are drinking enough by the colour of your urine, which should stay a very pale yellow to clear colour. You should also maintain a well balanced diet and eat foods in moderation. If stones continue to reform frequently and there is a proven metabolic problem certain diet restrictions and medication may be needed to help prevent further formation of stones.
While you are in hospital we will do everything we can to make your stay as comfortable as possible. The nursing and medical staff is always available to help with whatever needs you have. If you are worried about anything before or after your surgery, or if you have any further questions or would like more information, please do not hesitate to ask your nurse who will be more than happy to help you.
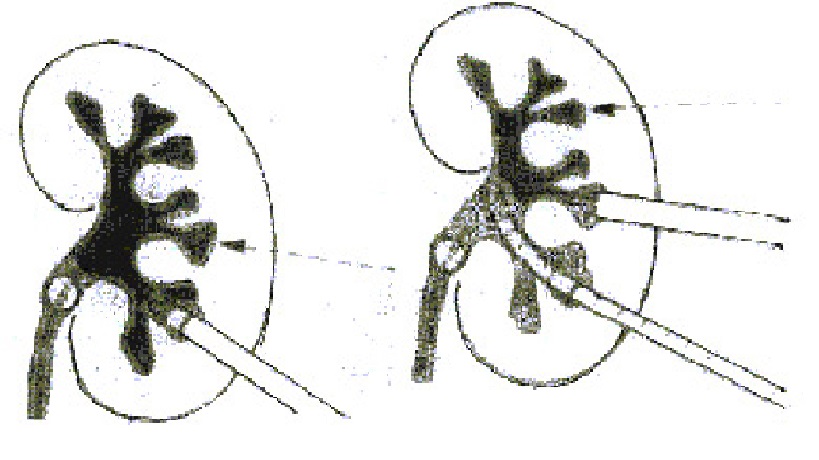
Diagram Illustrating How PCNL is Performed